
989 085 0037
779 868 0437
(whatsapp no.)
779 868 0437
(whatsapp no.)
MON - SAT
9:00AM to 1:00PM
4:00PM to 9:00PMSUN
9:00AM to 1:00PM
9:00AM to 1:00PM
4:00PM to 9:00PMSUN
9:00AM to 1:00PM

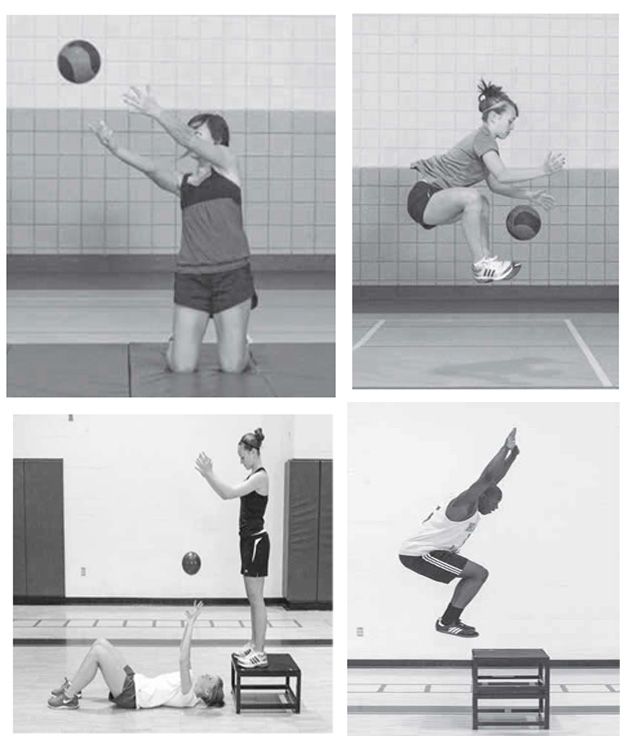
Plyometric exercise is a popular form of training used to improve athletic performance. It involves a stretch of the muscle-tendon unit immediately followed by a shortening of the muscle unit. This process of muscle lengthening followed by rapid shortening during the stretch-shortening cycle (SSC) is integral to plyometric exercise. The SSC process significantly enhances the ability of the muscle-tendon unit to produce maximal force in the shortest amount of time. These benefits have prompted the use of plyometric exercise as a bridge between pure strength and sport-related power and speed.
As plyometric training techniques have evolved, the description of this training and the related terminology have undergone a metamorphosis. Because the term plyometrics is a later creation in American training literature, much of the early physiological research on this type of training described it by other names. The term used by researchers in Italy, Sweden, and the Soviet Union for the type of muscle action involved was the stretch-shortening cycle. Coaches in these countries simply referred to the use of such exercises in their training programs as jump training. Based on original forms of training described by Yuri Verkhoshansky, the Russian national jump coach for track and field, plyometrics were originally developed as a shock method of training.
The Plyometrics exercises can be useful if administered carefully considering the capability of an individual.
Kinesio taping (KT) is a therapeutic taping technique developed by Dr. Kenzo Kase in Japan more than 25 years ago1. This technique is used as an alternative to athletic taping to support the fascia, muscles, and joints; however, unlike athletic taping, Kinesio Tape (KT) allows for unrestricted range of motion (ROM) and is also theorized to reduce the time for recovery from injury by decreasing pain and inflammation1. This unique taping method was popularized by the press at the Seoul Olympics in 19881. Since then, it has become a popular treatment modality, especially among athletes. Athletic trainers, physical therapists, and physicians have used this technique to facilitate healing after musculoskeletal injury1,2.
The KT is designed to mimic the approximate thickness and weight of skin and has elasticity of up to 30% to 40% over its resting length, which gives the tape unique properties1,3. This tape is also latex-free and features an adhesive that is 100% heat-activated acrylic1,3. The 100% cotton fibers allow for evaporation and fast drying, thereby ensuring that patients can wear the tape even in the shower or pool without the need for reapplication; this allows for a wear time of 3 to 5 days and makes the treatment more economical.

Type 2 diabetes is characterised by high levels of glucose in the blood, due to insulin resistance and relative insulin deficiency. Physical inactivity and hyper-caloric food are the main contributors to type 2 diabetes.
Poorly regulated blood glucose increases the patient’s risk of developing medical complications related to diabetes. These complications include heart disease, stroke, neuropathy, foot ulcers, kidney failure and eye disease. Lower blood glucose values are associated with a lower risk of complications1.
Diabetes mellitus is a leading cause of death and disability world wide2,3. Asia and the eastern Pacific region are particularly affected4-9. Nowhere is the diabetes epidemic more pronounced than in India as the World Health Organization (WHO) reports show that 32 million people had diabetes in the year 200010. The Diabetes Prevention Project dem¬onstrated that lifestyle modification, including intensive exercise, is more effective in preventing diabetes than pharmacological therapy, and high¬lighted the role of trained professionals in motivating people to follow lifestyle interventions. Similar results have been reported by the Malmö Study, the Da Qing Study, the Finnish Diabetes Prevention Study and the Wenying Study11.
Physiotherapy is a branch of rehabilitative health that uses specially designed exercises and equipment to help patients regain or improve their physical abilities.
The World Health Organization states that - "Physiotherapists assess, plan and implement rehabilitative programs that improve or restore human motor functions, maximize movement ability, relieve pain syndromes, and treat or prevent physical challenges associated with injuries, diseases and other impairments. They apply a broad range of physical therapies and techniques such as movement, ultrasound, heating, laser and other techniques. They may develop and implement programmes for screening and prevention of common physical ailments and disorders."
Physiotherapists offer evidence-based training interventions encompassing aerobic training and/or resistance training. Three meta-analyses showed that both of these training modalities are effective in lowering the blood glucose by 0.5-0.8% in HbA1c (blood glucose control)12-14.
Physiotherapists are able to help people plan an individualized exercise programme in order to main¬tain good blood glucose control and achieve optimal weight. Furthermore, physiotherapy leads to metabolic improvements even in the absence of weight loss, reducing the frequency of cardiovascular events and improving life expectancy. Effective exercise counselling ensures both cardio-respiratory and musculoskel¬etal fitness11.
In patients with type 2 diabetes aerobic training may increase aerobic capacity by 15% and resistance training may increase the muscle strength by 19%. Increased aerobic capacity and muscle strength is associated with improved physical performance which has great relevance to the increasing number of elderly patients with type 2 diabetes. Optimal training interventions may include training sessions three times a week for a minimum of 12 weeks. However, these interventions may be planned in different ways and include non-supervised training sessions.
Physiotherapists may also deliver beneficial interventions with lower levels of physical activity. While not all patients are attracted to aerobic or resistance training, some may prefer physical activities outside the gym. Brisk walking is an alternative that has been shown to be effective in reducing blood glucose in patients with type 2 diabetes15,16.
Physiotherapists play a crucial role in type 2 diabetes treatment programs. These structured programs encompass supervised physical training, patient counselling and patient education. They have a wealth of experience of training patients suffering from various symptoms and diagnoses. Once the non-diabetic conditions are identified and the training programs adapted, the patients can engage safely in training sessions.
The effect of long-term physical training on blood glucose is at the same level as anti-diabetic drug or insulin therapy in patients with type 2 diabetes. Thus, if physical activity interventions are accepted by the patients, training may reduce the use of medication and thereby become a cost-saving initiative.
A 1% reduction in blood glucose control (HbA1c) is associated with a risk reduction of 21% of any complication related to diabetes1. Physical training is recognised as a method of treatment to reduce the blood glucose. Furthermore, training also reduces other morbidity and mortality risk factors suggesting that such interventions save costs on a long term basis.
Finally, training given to patients with type 2 diabetes may also be effective in combating other pre-existing health problems, including loss of bone strength, musculoskeletal pain and reduced mental health.
Physical training is a cornerstone in the treatment of type 2 diabetes. Training programs are cost-effective; they prevent medical complications and reduce the mortality risk. Physiotherapists play an important role in the treatment of type 2 diabetes by leading evidence-based training programs. The importance of having physiotherapist-led training programs is emphasised by the patients’ individual impairments and other disorders.
References

“You have got me rid of the Spinal Surgery” I was told by a surgeon to undergo spinal operation for my back and left leg radiating pain problem. But your scientific approach and proper guidance in Physiotherapy and Hydrotherapy have got me rid of surgery. Today I can swim, I can ride my bike and able to do my daily activities. Thank you.